
Zirconia - is it finally here?This 70 year old patient presented with a chief complaint of “I don’t like the looks of my front teeth”. His medical history was non-contributory. He reported that he had lost his front tooth more than 30 years ago and the fixed partial denture was placed at that time. Clinical exam revealed a cantilever bridge with a ¾ gold crown abutment on #8 and a resin bonded to gold pontic #9 (Fig 1). Figure 1  Teeth #7, 10 both had significant lingual attrition into dentin. Teeth #7/27 were end to end, tooth #8 was end to end with #26 and in cross bite with #25. Pontic #9 and tooth #10 were both in cross bite. Teeth #25 and 26 had significant incisal edge attrition and teeth # 23, 24 were supererupted . The pontic area presented as a Siebert Class I defect, with minimal loss of facial contour. The esthetic exam revealed minimal incisal display in full smile; in fact, the patient had lost the skill to smile. Treatment options were discussed with the patient. He was advised that it wasn’t possible to provide an esthetic solution for his unesthetic upper fixed partial denture with his aberrant occlusal relationship. The patient understood and accepted the need to have orthodontic realignment of the teeth. We also discussed an implant in the edentulous site versus a fixed partial denture. Based on the restorative needs of the adjacent teeth, the patient chose the fixed partial denture option. The orthodontic treatment required approximately 8 months to complete (Fig 2). Figure 2  After de-banding, tooth #7 was prepared for a zirconia crown, and teeth #8,10 were prepared for a zirconia fixed partial denture. No ovate pontic site preparation was accomplished prior to the day the restorations were inserted. On insertion day, the ovate pontic site was prepared with a KS-5 bur (Brasseler) (Figs. 3,4). Figure 3 Figure 4
The fixed partial denture was tried in, but did not completely seat. The area in the ovate pontic site that was preventing complete seating was removed with the KS-5 bur, and the fixed partial denture was completely seated (Fig 5). Figure 5  It was then removed and the ovate pontic site was bone sounded to insure that a minimum of 2 mm of soft tissue remained from the base of the ovate pontic site to the alveolar bone (Fig 6 different case). Figure 6 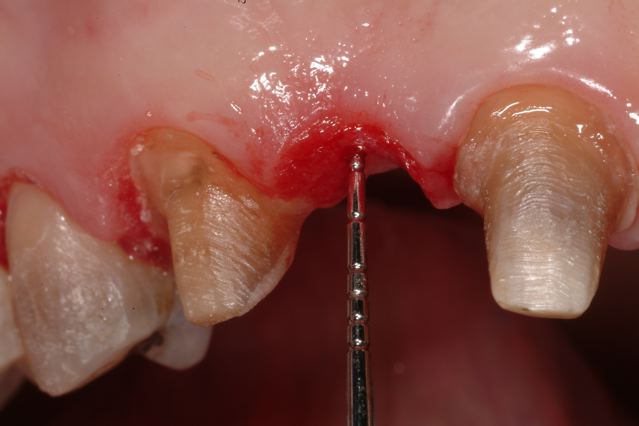 Figure A
If the distance was less than 2 mm, the remaining soft tissue as well as alveolar bone in the pontic site would have been removed using the KS-5 bur. During the try-in of the fixed partial denture, it was noted that the gingival embrasure between the pontic and the abutment #10 was significantly open, resulting in an esthetic compromise (Fig 7). Figure 7  In order to determine if the gingival embrasure would fill with tissue over time, the area between the pontic and crown was bone sounded (Fig 8). Figure 8  If the distance from the bottom of the contact to the alveolar bone is less than 5 mm, the probability of gingival fill of the embrasure is very high. In this case the distance was 5 mm; therefore, the decision was made to cement the fixed partial denture. The crown and the zirconia bridge were cemented with a resin modified glass ionomer cement, Rely X luting cement (3M). At the 2 week post-op photo, the papilla is already beginning to fill the open gingival embrasure (Fig 9). Figure 9  I have just dipped my toe in the world of zirconia as a replacement for ceramometal for the past 6 months. With a few technical caveats which Dene will discuss, it appears that zirconia is the deal. In my opinion, the anterior esthetics are superior to ceramometal. Time will tell about the longevity.
William Robbins, D.D.S., M.A. 1202 East Sonterra Blvd. Suite 402 San Antonio, Texas 78258 Phone: (210) 341-4409 Fax: (210) 403-9387 E-mail: [email protected] website: www.beckelrobbinsdds.com website: www.coredentistry.com website: www.surgeryrr.com
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
Dental Street Blog
Categories
All
Archives
November 2022

|



 RSS Feed
RSS Feed
|
|
HoursM-TH: 7am - 4pm
PST |
Telephone425-251-3535
|
|
Copyright © 2011 LeBeau all rights reserved Website created by: Cuddy Connections LLC.