
Is There a New Gold Standard for Impressioning in Indirect Restorative Dentistry? Dr. Brian Schroder Elastomeric Impressions Are there times that you feel as though you have knocked the ball out of the park only to end up striking out? The use of impression material can challenge the best of any doctor’s efforts. I’ve been a player in the game of general dentistry for 32 years, during which I have navigated and incorporated the evolution of elastomeric impression materials. I have used:
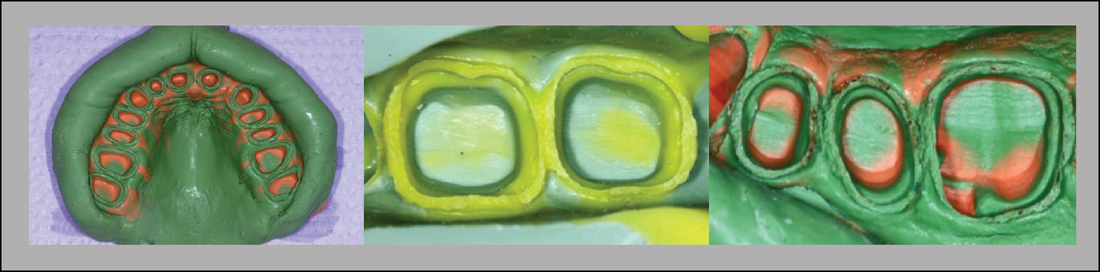 Make no mistake; the quality of impression materials available today for use in restorative dentistry is superior to any other time in our professional careers. Without question we can create outstanding restorations using conventional impression materials. However, I must tell you, there was an element of frustration that arose each time I had a case (regardless of my efforts) where the material was not placed ideally only to have to remake my impression. Or worse, despite the appearance of excellence in the impression, the final restorations were not clinically acceptable. Perhaps margins were not ideal, interproximal contacts were open or tight, occlusion was high, and/or the restorations did not intimately fit the preparations. In retrospect, I believe that the reason for these infrequent but significant challenges were a direct cause of the unavoidable flaws of the conventional impressioning systems. As I considered the multitude of steps from beginning to end, it became clear that there were significant opportunities to incorporate distortion and inaccuracies into the process, a few of these were:  Even if all of these steps worked perfectly, think of the post impressioning steps this impression must go through to arrive at a gypsum die stone cast, upon which the laboratory technician works his or her magic:  Digital Impressions My frustration with the impressioning process encouraged me to find a better way. Enter digitization. It occurred to me that computers belonged in restorative dentistry. The reason? They increase efficiency and accuracy. What at first was a tremendous paradigm shift has now become the mainstay of my restorative practice. I have been using a dedicated digital impressioning system (not a chairside milling system) since January 2009 and have found that it eliminates nearly all of the challenges of conventional systems. The digital impressioning system creates new solutions to old issues and has allowed for:  Obstacles to successful impressioning are reduced to one concern, isolation. This is no small challenge. It is important to note that digital systems do not excuse us from following excellent technique in the biomechanics of our craft; but they have the ability to replace parts of the process. Suffice to say, if the computer can see the margins of the preparations and all critical areas, in this practitioners experience (which includes over 2000 restorations in over 1300 patients), it can capture them accurately and permanently. There are many digital systems in the commercial marketplace and my purpose is not to endorse any of them. Those of you who know me have heard me say many times: “Success is OPERATOR DEPENDENT long before it is PRODUCT DEPENDENT”. In my practice I began this adventure with the LAVA Chairside Oral Scanner. When the COS was phased out I was introduced to the first edition of Tru Def and found it to be insufficient to meet my needs. I have recently transitioned to the latest iteration of Tru Def and find it fully capable of replacing impression material entirely in all tooth borne indirect restorations, as well as many implant-supported cases. This includes everything from single unit cases to full arch, and multi-unit restorations. The video links and photos that follow will demonstrate a single unit case involving a partial coverage eMax crown for tooth #4.  The second retraction cord is removed, clearly visible margins and preparations are verified, a very light reflective medium is applied. The scanner is introduced and passed over the areas that one would want captured in a conventional impression. Note that the operator looks at the computer screen while scanning and confirms data uptake as the “cast” is created. (Scan preparation video below).  Once the entire operative arch is scanned, the opposing arch and jaw relation are then scanned. Note in the video of the jaw relation that the patient is guided into maximum intercuspal position and the buccal surfaces of the teeth are recorded. The computer then has the ability to orient the maxilla and mandible into articulated replicas of the teeth. (Jaw relation recording video below). One distinct advantage of the digital process is the ability to review all captured data up to 20x magnification prior to prescription and signing. Problems can be detected, changes can be made, and then the case can be rescanned. No more guess work! (Video of scan preview below).
Next, an online prescription is completed and the case is forwarded to the laboratory of your choice. The laboratory processes are detailed in these photos. 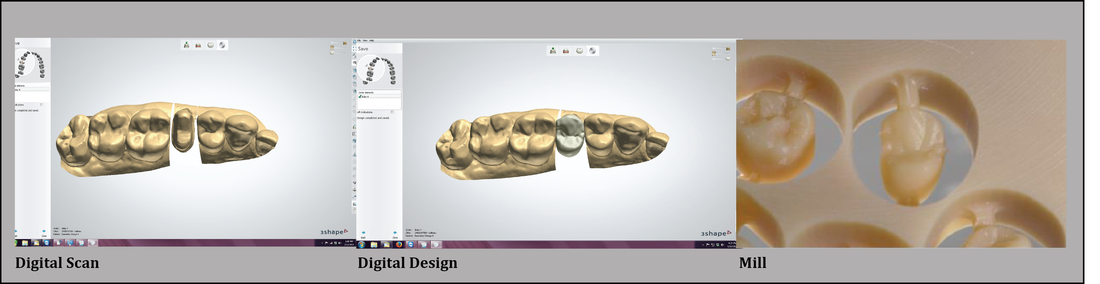 The final restoration required very slight adjustment of the distal interproximal contact, and an equally slight reduction of the occlusion on the distolingual cuspal incline. My experience with this system has been a positive one. Certainly the learning curve requires a degree of determination, and technology is not without challenges, but this change is a step in a positive direction. 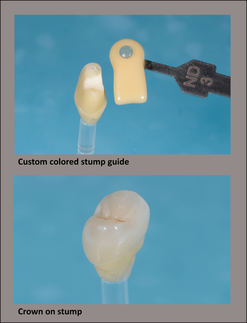 In my opinion, on its best day impression material has the ability to be as good as a digital impression, only computers don’t have bad days. Overall, impressioning is difficult, isolation is the greatest challenge, conventional systems are filled with errors, and digital systems eliminate most of those errors. Thankfully, using a dedicated digital impressioning system has nearly eliminated my obstacles with impressions. Now we can knock the ball out of the park without the worry of striking out! Digital impressioning is certainly my new gold standard. Batter up? 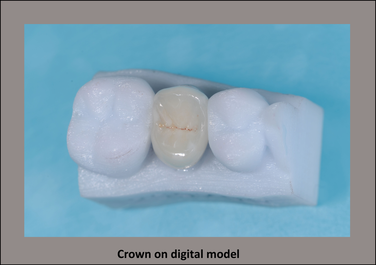  Sincerely,
Dr. Brian Schroder Scan Video JRR Video Preparation Video Don’t forget to visit our website for more information Comments are closed.
|
Dental Street Blog
Categories
All
Archives
November 2022

|

 RSS Feed
RSS Feed
|
|
HoursM-TH: 7am - 4pm
PST |
Telephone425-251-3535
|
|
Copyright © 2011 LeBeau all rights reserved Website created by: Cuddy Connections LLC.